Abstract
Introduction: Autism spectrum disorder (ASD) is a neurodevelopmental condition characterized by substantial phenotypic and genetic heterogeneity. The recent application of person-centered computational models has allowed the identification of novel clinical subtypes with distinct genetic underpinnings. Objective: To review recent literature on the classification of ASD subtypes through integrative approaches combining clinical, phenotypic, and genomic data, with emphasis on diagnostic, prognostic, and therapeutic implications. Methods: A narrative review of articles published between 2018 and 2024 was conducted in PubMed, Scopus, and Web of Science, using search terms such as “autism subtypes,” “phenotypic clustering,” “genetic architecture in ASD,” and “precision medicine in autism.” Eligible studies included original research, systematic reviews, and meta-analyses. Results: Recent studies have identified at least four robust clinical-biological ASD subtypes using finite mixture modeling and person-centered analyses: (1) social and behavioral challenges, (2) mixed ASD with developmental delay, (3) moderate challenges, and (4) broadly affected subtype. Each group presents distinctive patterns in symptoms, comorbidities, developmental trajectories, and genetic architecture. Both de novo mutations and inherited variants play key roles in molecular differentiation among subtypes. Conclusions: The identification of more homogeneous subgroups within the autism spectrum represents a crucial step toward personalized medicine in ASD. Emerging clinical tools derived from these classifications may enhance prognosis prediction and guide tailored interventions.
Keywords
Autism Spectrum Disorder, Clinical Subtypes, Phenotypic Clustering, Genetic Variants, Personalized Medicine
1. Introduction
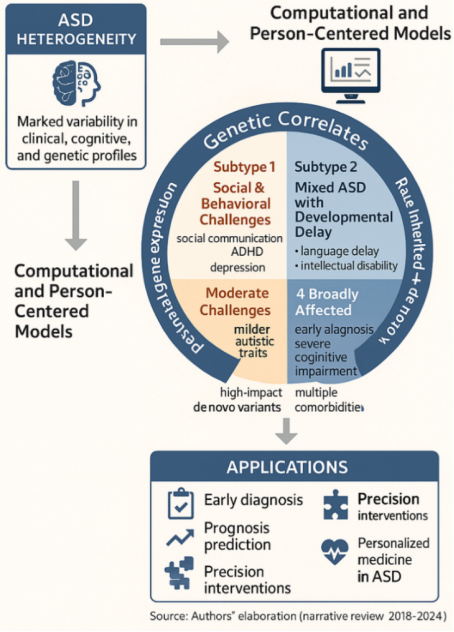
Autism spectrum disorder (ASD) is a neurodevelopmental condition defined by developmental speech delay, persistent deficits in social communication, restricted interests, and repetitive behaviors, together with a striking heterogeneity in clinical, cognitive, and functional manifestations
| [1] | Lord C, Elsabbagh M, Baird G, Veenstra-VanderWeele J. Autism spectrum disorder. Lancet. 2018; 392(10146): 508-520. |
[1]
. Its global prevalence has risen significantly in recent decades, affecting diverse populations and emphasizing the importance of studying regional and ethnic genetic contributions to its pathogenesis, stimulating research into its biological bases and clinical classification
| [2] | Al-Sarraj Y, Taha RZ, Al-Dous E, Ahram D, Abbasi S, Abuazab E, et al. The genetic landscape of autism spectrum disorder in the Middle Eastern population. Front Genet. 2024; 15: 1363849. https://doi.org/10.3389/fgene.2024.1363849 |
[2]
.
From a genetic perspective, ASD is highly complex, involving hundreds of associated genes that range from common low-effect variants to highly penetrant de novo mutations
| [3] | Matoba N, Liang D, Sun H, Aygün N, McAfee J, Davis JE, et al. Common genetic risk variants identified in the SPARK cohort support DDHD2 as a candidate risk gene for autism. Transl Psychiatry. 2020; 10: 265. https://doi.org/10.1038/s41398-020-00953-9 |
[3]
. Studies in large cohorts, including the
SPARK initiative | [3] | Matoba N, Liang D, Sun H, Aygün N, McAfee J, Davis JE, et al. Common genetic risk variants identified in the SPARK cohort support DDHD2 as a candidate risk gene for autism. Transl Psychiatry. 2020; 10: 265. https://doi.org/10.1038/s41398-020-00953-9 |
| [5] | Simons Foundation Autism Research Initiative. About SPARK: Simons Foundation Powering Autism Research for Knowledge 2025 Apr 8 (cited 2025 Jul 19). Available from: https://sparkforautism.org/portal/page/about-spark/ |
[3, 5]
, and the
Simons Simplex Collection (SSC) have been instrumental in identifying risk genes such as DDHD2
| [3] | Matoba N, Liang D, Sun H, Aygün N, McAfee J, Davis JE, et al. Common genetic risk variants identified in the SPARK cohort support DDHD2 as a candidate risk gene for autism. Transl Psychiatry. 2020; 10: 265. https://doi.org/10.1038/s41398-020-00953-9 |
[3]
and in demonstrating that phenotypic heterogeneity is strongly correlated with distinct genetic architectures
. (See
Figure 1).
Genome-wide association studies further support the role of common variants
| [6] | Grove J, Ripke S, Als TD, Mattheisen M, Walters RK, Won H, et al. Identification of common genetic risk variants for autism spectrum disorder. Nat Genet. 2019; 51(3): 431-444. https://doi.org/10.1038/s41588-019-0344-8 |
[6]
, while large-scale exome sequencing has revealed developmental and functional changes in neurobiology attributable to rare and de novo mutations
| [7] | Satterstrom FK, Kosmicki JA, Wang J, Breen MS, De Rubeis S, An JY, et al. Large-scale exome sequencing study implicates both developmental and functional changes in the neurobiology of autism. Cell. 2020; 180(3): 568-584.e23. https://doi.org/10.1016/j.cell.2019.12.036 |
[7]
. Synaptic, transcriptional, and chromatin-related genes have also been implicated, underscoring the complexity of molecular mechanisms involved
| [8] | De Rubeis S, He X, Goldberg AP, Poultney CS, Samocha K, Cicek AE, et al. Synaptic, transcriptional and chromatin genes disrupted in autism. Nature. 2014; 515(7526): 209-215. https://doi.org/10.1038/nature13772 |
[8]
. However, this extensive genetic repertoire has not easily translated into operational clinical classifications, largely due to the broad phenotypic variability observed among individuals.
The clinical heterogeneity of ASD has led to the proposal of multiple biological and clinical subtypes identifying shared core symptoms. Recent conceptual frameworks, supported by person-centered computational models, employing computational tools and statistical models, highlight the possibility of decomposing phenotypic variability into more homogeneous subgroups with specific genetic underpinnings
| [4] | Wigdor EM, Gandal MJ, Parikshak NN, et al. Genetic correlates of phenotypic heterogeneity in autism. Nat Genet. 2022; 54: 212-224. https://doi.org/10.1038/s41588-022-01072-5 |
| [9] | Al-Beltagi M. Pre-autism: Advancing early identification and intervention in autism. World J Clin Cases. 2024; 12(34): 6748-6753. https://doi.org/10.12998/wjcc.v12.i34.6748 |
| [10] | Litman A, Sauerwald N, Green Snyder L, Foss-Feig J, Park CY, Hao Y, Dinstein I, Theesfeld CL, Troyanskaya OG. Decomposition of phenotypic heterogeneity in autism reveals underlying genetic programs. Nat Genet. 2025. https://doi.org/10.1038/s41588-025-02224-z |
[4, 9, 10]
. This movement toward identifying
biological subtypes has been recognized not only in research articles but also in clinical and scientific reports, 11 reinforcing its translational potential.
At the same time, increasing emphasis has been placed on early identification of “pre-autism” features to allow timely intervention. The concept of pre-autism has been proposed as an emerging stage in which risk markers can be recognized before full diagnostic criteria are met, thereby opening a window for preventive care
.
Evidence also demonstrates that early intervention significantly improves outcomes in social communication and overall development. A meta-analysis confirmed positive effects of structured programs
| [13] | Fuller EA, Kaiser AP. The effects of early intervention on social communication outcomes for children with autism spectrum disorder: a meta-analysis. J Autism Dev Disord. 2020; 50(5): 1683-1698. https://doi.org/10.1007/s10803-019-03927-z |
[13]
, and subsequent reviews have highlighted the benefits of early therapeutic approaches in children at high likelihood of ASD
| [14] | Franz L, Goodwin C, Rieder A, Metheis M, Damiano DL. Early intervention for very young children with or at high likelihood for autism spectrum disorder: an overview of reviews. Dev Med Child Neurol. 2022; 64(9): 1063-1073. https://doi.org/10.1111/dmcn.15258 |
[14]
. Systematic reviews emphasize that early interventions, even before a formal diagnosis, contribute to improved adaptive skills and communication
| [15] | French L, Kennedy EM. Early intervention for infants and young children with, or at-risk of, autism spectrum disorder: A systematic review. J Child Psychol Psychiatry. 2018; 59(4): 444-458. https://doi.org/10.1111/jcpp.12828 |
[15]
. Furthermore, specific models such as the
Early Start Denver Model have been examined within the framework of applied behavioral analysis (ABA), with evidence supporting their effectiveness in early developmental stages
.
The integration of genetic and phenotypic data is crucial for refining classification. Cohort-based analyses show that phenotypic heterogeneity has strong genetic correlates
, and conceptual reviews highlight the challenges of defining “problem behaviors” in early childhood, which remain inconsistently operationalized across intervention studies
| [18] | Lin A, Rorvik A, et al. Conceptualizing and measuring ‘problem behavior’ in early childhood in ASD: a systematic review. JCPP Res Pract. 2025; ahead of print. https://doi.org/10.1111/jcpp.14177 |
[18]
. Advances in machine learning have begun to facilitate the integration of clinical phenotypes with transcriptomic data, increasing screening precision and improving the identification of biologically meaningful subgroups
| [19] | Bedford R, Waldmann S, et al. Machine learning of clinical phenotypes facilitates autism screening: insights from AGRE and transcriptomics. Sci Rep. 2025; 15(1): 95291. https://doi.org/10.1038/s41598-025-95291-5 |
[19]
.
Finally, systematic reviews and meta-analyses confirm that structured early intervention programs yield moderate but consistent benefits across developmental domains
| [20] | Gómez-Cotilla R, López-de-Uralde-Selva MA, Valero-Aguayo L. Efficacy of early intervention programmes: systematic review and meta-analysis. Psicol Educ. 2024; 30(1): 1-10. https://doi.org/10.5093/psed2024a1 |
[20]
. Together, these findings underscore the need to bridge biological classification with early, targeted clinical strategies.
The aim of this review is to synthesize the most recent findings on ASD subtype classification, integrating clinical and genetic evidence, with emphasis on its applicability to personalized medicine and to prognostic and therapeutic approaches.
Figure 1. Biological and Clinical Subtypes in Autism Spectrum Disorder: Phenotypic and Genetic Advances.
2. Materials and Methods
This review follows a qualitative, narrative, and descriptive approach in accordance with the SANRA (Scale for the Assessment of Narrative Review Articles) criteria. The objective was to compile and critically analyze recent evidence on the identification of clinical-biological subtypes of autism spectrum disorder (ASD) using integrative methodologies that combine phenotypic and genetic data.
2.1. Search Strategy and Selection Workflow
The literature search was conducted in the PubMed, Scopus, and Web of Science databases, covering the period between January 2018 and April 2024. The following English keywords were used, combined with Boolean operators: “autism subtypes,” “phenotypic clustering,” “person-centered modeling in autism,” “genetic architecture in ASD,” “ASD precision medicine,” and “SPARK autism cohort.”
Inclusion criteria:
1) Original articles from observational studies (cohort, cross-sectional, or retrospective), systematic reviews, meta-analyses, and relevant narrative reviews.
2) Studies published in English or Spanish.
3) Research focused on phenotypic or genetic classification of ASD.
Exclusion criteria:
1) Case reports, letters to the editor, brief communications, editorials, or non-peer-reviewed articles.
2) Studies including exclusively adult populations or lacking a specified clinical diagnosis.
The selection process was performed in three stages: (1) title and abstract screening to exclude non-relevant articles, (2) full-text critical reading to ensure alignment with the study objectives, and (3) qualitative evaluation of methodological quality and translational relevance.
A total of 38 full-text articles were included, originating from large cohort studies such as SPARK and the Simons Simplex Collection (SSC), as well as research focused on phenotypic analysis, subgroup identification, and genomic correlation.
2.2. Study Appraisal
All included studies were appraised qualitatively according to five domains: design clarity and appropriateness, internal validity, sample characterization, cohort data quality, and clinical or translational relevance. Each article was independently reviewed by two authors, and any discrepancies were resolved through discussion until consensus was reached. Given the heterogeneity of study designs, no quantitative scoring or risk-of-bias tools were applied; instead, emphasis was placed on interpretive and methodological rigor.
2.3. Data Extraction and Thematic Synthesis
Extracted data were organized into thematic matrices and qualitatively analyzed across four domains:
1) classification of ASD subtypes,
2) distinctive clinical and behavioral features,
3) differential genetic or molecular profiles, and
4) applications in precision or personalized medicine.
Data extraction followed a dual-reviewer process, with reconciliation of discrepancies and integration of findings through thematic coding. This narrative synthesis enabled identification of conceptual overlaps, methodological trends, and gaps in the literature. The choice of a narrative approach—rather than a systematic or meta-analytic design—is justified by the exploratory and heterogeneous nature of the available evidence.
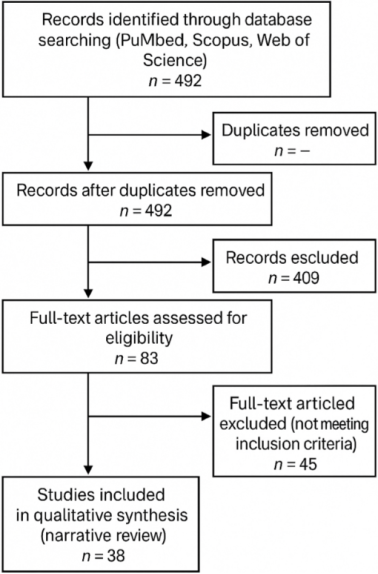
Figure 2. PRISMA flow diagram of the study selection process for the narrative review.
3. Results
Following the predefined inclusion and exclusion criteria, 492 initial records were identified in the databases searched. After screening titles and abstracts, 409 articles were excluded for irrelevance, duplication, or being editorials. Eighty-three full-text articles were assessed for eligibility, and 38 were ultimately included in the qualitative review (see
Figure 2).
The selected studies comprised observational research, computational analyses of large cohorts (mainly SPARK and the Simons Simplex Collection), as well as systematic reviews and recent meta-analyses addressing phenotypic and genomic classification of ASD.
From the thematic analysis, the following main findings were identified:
1)
Person-centered phenotypic classification: Multiple studies converged on the use of finite mixture models to identify four consistent clinical subtypes within the autism spectrum
. (see
Figure 3):
a) Social and Behavioral Challenges: Greater impairment in social communication, anxiety, depression, and ADHD, without significant developmental delay.
b) Mixed ASD with Developmental Delay: Predominantly language impairment, intellectual disability, and motor disorders.
c) Moderate Challenges: Milder autistic symptoms, with near-typical developmental trajectories.
d)
Broadly Affected: Severe cognitive impairment, early diagnosis, and multiple psychiatric comorbidities
.
Person-centered computational models—such as latent class analysis and finite mixture modeling—represent data-driven clustering methods that estimate latent subgroups based on joint distributions of symptoms and comorbidities, assigning probabilistic class membership to each participant. These approaches identify hidden phenotypic structures within heterogeneous ASD populations and enable external validation through independent cohorts or convergent biomarker data. When combined with genetic and neuroimaging datasets, they enhance the biological interpretability and translational value of identified subtypes.
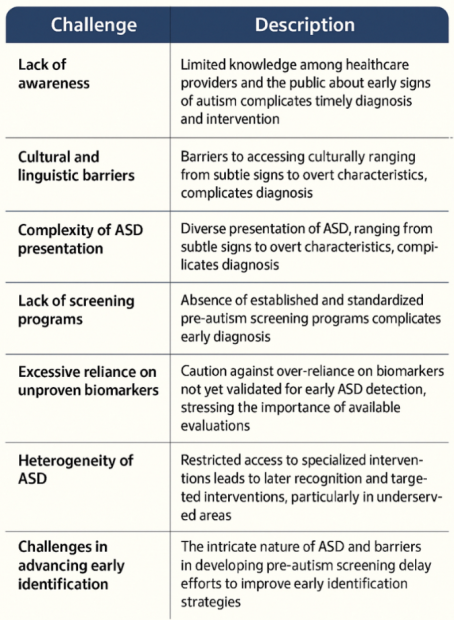
Figure 3. Challenges for Early Diagnosis and intervention in Autism Spectrum Disorder.
2)
Genetic correlations among subtypes: Clear differences in the burden and type of genetic variants were observed
:
a) The
Broadly Affected subtype showed the highest prevalence of high-impact de novo variants
| [6] | Grove J, Ripke S, Als TD, Mattheisen M, Walters RK, Won H, et al. Identification of common genetic risk variants for autism spectrum disorder. Nat Genet. 2019; 51(3): 431-444. https://doi.org/10.1038/s41588-019-0344-8 |
| [7] | Satterstrom FK, Kosmicki JA, Wang J, Breen MS, De Rubeis S, An JY, et al. Large-scale exome sequencing study implicates both developmental and functional changes in the neurobiology of autism. Cell. 2020; 180(3): 568-584.e23. https://doi.org/10.1016/j.cell.2019.12.036 |
| [8] | De Rubeis S, He X, Goldberg AP, Poultney CS, Samocha K, Cicek AE, et al. Synaptic, transcriptional and chromatin genes disrupted in autism. Nature. 2014; 515(7526): 209-215. https://doi.org/10.1038/nature13772 |
[6-8]
.
b) The
Mixed with Developmental Delay subtype presented a combination of de novo and rare inherited variants, suggesting stronger hereditary contributions
| [6] | Grove J, Ripke S, Als TD, Mattheisen M, Walters RK, Won H, et al. Identification of common genetic risk variants for autism spectrum disorder. Nat Genet. 2019; 51(3): 431-444. https://doi.org/10.1038/s41588-019-0344-8 |
| [7] | Satterstrom FK, Kosmicki JA, Wang J, Breen MS, De Rubeis S, An JY, et al. Large-scale exome sequencing study implicates both developmental and functional changes in the neurobiology of autism. Cell. 2020; 180(3): 568-584.e23. https://doi.org/10.1016/j.cell.2019.12.036 |
| [11] | Wendling P. Four biologically, clinically distinct autism subtypes identified. Medscape Medical News. 2025 Jul 16 (cited 2025 Jul 19). Available from: https://www.medscape.com/viewarticle/four-biologically-clinically-distinct-autism-subtypes-2025a1000isk |
[6, 7, 11]
.
c) In the
Social and Behavioral subtype, affected genes were predominantly expressed postnatally, correlating with later onset and preserved developmental milestones
| [4] | Wigdor EM, Gandal MJ, Parikshak NN, et al. Genetic correlates of phenotypic heterogeneity in autism. Nat Genet. 2022; 54: 212-224. https://doi.org/10.1038/s41588-022-01072-5 |
| [10] | Litman A, Sauerwald N, Green Snyder L, Foss-Feig J, Park CY, Hao Y, Dinstein I, Theesfeld CL, Troyanskaya OG. Decomposition of phenotypic heterogeneity in autism reveals underlying genetic programs. Nat Genet. 2025. https://doi.org/10.1038/s41588-025-02224-z |
| [11] | Wendling P. Four biologically, clinically distinct autism subtypes identified. Medscape Medical News. 2025 Jul 16 (cited 2025 Jul 19). Available from: https://www.medscape.com/viewarticle/four-biologically-clinically-distinct-autism-subtypes-2025a1000isk |
[4, 10, 11]
.
3)
External validation: Subtypes were replicated in the independent
Simons Simplex Collection, characterized by clinician-verified diagnoses, supporting the robustness of the proposed model
.
4)
Clinical applications: Several authors emphasized the potential of these classifications for clinical stratification, the development of phenotype-based diagnostic tools, and the design of more personalized interventions within the framework of precision medicine in ASD
| [9] | Al-Beltagi M. Pre-autism: Advancing early identification and intervention in autism. World J Clin Cases. 2024; 12(34): 6748-6753. https://doi.org/10.12998/wjcc.v12.i34.6748 |
| [13] | Fuller EA, Kaiser AP. The effects of early intervention on social communication outcomes for children with autism spectrum disorder: a meta-analysis. J Autism Dev Disord. 2020; 50(5): 1683-1698. https://doi.org/10.1007/s10803-019-03927-z |
| [14] | Franz L, Goodwin C, Rieder A, Metheis M, Damiano DL. Early intervention for very young children with or at high likelihood for autism spectrum disorder: an overview of reviews. Dev Med Child Neurol. 2022; 64(9): 1063-1073. https://doi.org/10.1111/dmcn.15258 |
[9, 13, 14]
.
Overall, the findings highlight a convergent trend in current literature toward integrative classifications of ASD that combine clinical, behavioral, and genetic data, with direct impact on etiological understanding and therapeutic planning.
4. Discussion of Results
The evidence reviewed confirms a growing trend toward decomposing Autism Spectrum Disorder (ASD) into more homogeneous clinical and biological subtypes. Person-centered methodologies and multidomain phenotypic analyses have enabled significant stratification beyond traditional approaches based solely on global behavioral symptoms.
Large cohorts such as SPARK and the Simons Simplex Collection (SSC) demonstrate that finite mixture models identify subtypes distinguished not only by symptom severity but also by comorbidities, diagnostic timing, cognitive development, and—critically—underlying genetic variants
. This represents a step toward precision medicine, linking observable phenotypes with specific biological mechanisms.
Notably, recognition that subtypes like Social and Behavioral Challenges involve mutations expressed primarily postnatally
suggests clinical relevance of genetic timing for prognosis and intervention. In contrast, Broadly Affectedsubtypes, with high-impact de novo variants
| [4] | Wigdor EM, Gandal MJ, Parikshak NN, et al. Genetic correlates of phenotypic heterogeneity in autism. Nat Genet. 2022; 54: 212-224. https://doi.org/10.1038/s41588-022-01072-5 |
| [6] | Grove J, Ripke S, Als TD, Mattheisen M, Walters RK, Won H, et al. Identification of common genetic risk variants for autism spectrum disorder. Nat Genet. 2019; 51(3): 431-444. https://doi.org/10.1038/s41588-019-0344-8 |
| [7] | Satterstrom FK, Kosmicki JA, Wang J, Breen MS, De Rubeis S, An JY, et al. Large-scale exome sequencing study implicates both developmental and functional changes in the neurobiology of autism. Cell. 2020; 180(3): 568-584.e23. https://doi.org/10.1016/j.cell.2019.12.036 |
| [10] | Litman A, Sauerwald N, Green Snyder L, Foss-Feig J, Park CY, Hao Y, Dinstein I, Theesfeld CL, Troyanskaya OG. Decomposition of phenotypic heterogeneity in autism reveals underlying genetic programs. Nat Genet. 2025. https://doi.org/10.1038/s41588-025-02224-z |
[4, 6, 7, 10]
, are associated with severe deficits and early diagnosis. These findings reinforce the view that ASD is not a linear spectrum of severity but a constellation of discrete neurobiological trajectories.
Validation in external cohorts further strengthens reproducibility, although methodological limitations remain, including reliance on self-reported data in some cohorts and limited ethnic and cultural diversity.
Clinically, advances in phenotypic-genetic classification create opportunities for automated clinical tools to assign subtypes, leveraging routinely collected data
| [10] | Litman A, Sauerwald N, Green Snyder L, Foss-Feig J, Park CY, Hao Y, Dinstein I, Theesfeld CL, Troyanskaya OG. Decomposition of phenotypic heterogeneity in autism reveals underlying genetic programs. Nat Genet. 2025. https://doi.org/10.1038/s41588-025-02224-z |
| [12] | Cortese S, Bellato A, Gabellone A, Marzulli L, Matera E, Parlatini V, et al. (2024). Latest clinical frontiers related to autism diagnostic strategies. Cell Reports Medicine, 6(2), 101916. https://doi.org/10.1016/j.xcrm.2024.101916 |
[10, 12]
. Such tools could guide targeted interventions from early stages, though their implementation will require validation, clinician training, and integration into health systems.
Recent reviews also highlight challenges in intervention research. For example, a systematic analysis of non-pharmacological interventions in autistic children under eight years revealed lack of consensus on which behaviors to target, underscoring the need for clearer conceptual frameworks and culturally sensitive approaches
| [18] | Lin A, Rorvik A, et al. Conceptualizing and measuring ‘problem behavior’ in early childhood in ASD: a systematic review. JCPP Res Pract. 2025; ahead of print. https://doi.org/10.1111/jcpp.14177 |
[18]
. Moreover, machine-learning approaches integrating ADI-R data with molecular information improved screening accuracy and showed stronger genotype-phenotype concordance, supporting a phenotype-first strategy
| [19] | Bedford R, Waldmann S, et al. Machine learning of clinical phenotypes facilitates autism screening: insights from AGRE and transcriptomics. Sci Rep. 2025; 15(1): 95291. https://doi.org/10.1038/s41598-025-95291-5 |
[19]
.
Meta-analyses confirm that early developmental interventions yield moderate benefits (d = 0.45)
| [20] | Gómez-Cotilla R, López-de-Uralde-Selva MA, Valero-Aguayo L. Efficacy of early intervention programmes: systematic review and meta-analysis. Psicol Educ. 2024; 30(1): 1-10. https://doi.org/10.5093/psed2024a1 |
[20]
, yet emphasize the need for standardized, long-term, and comparative studies. (See
Table 1)
Table 1. Strategies to Improve Early Diagnosis and Intervention in Autism Spectrum Disorder.
Key Area | Action to be Taken |
Awareness | Develop educational programs for healthcare professionals, teachers, and the general public to recognize early signs of autism. |
Culturally appropriate resources | Produce and distribute materials adapted culturally and linguistically to facilitate equitable access to services in diverse communities. |
Screening implementation | Design and establish standardized early detection systems to identify cases in a timely manner and facilitate early interventions. |
Biomarker research | Advance scientific validation of biomarkers useful in early ASD stages, avoiding premature use without sufficient clinical evidence. |
Personalized detection | Promote evaluations tailored to the variability of ASD manifestations, considering the specific needs of each individual. |
Access to specialized services | Improve the availability of services and therapies in resource-limited regions to reduce delays in diagnosis and intervention. |
Multisectoral collaboration | Foster partnerships among healthcare professionals, researchers, and technology sectors to innovate in early detection and intervention tools. |
This supports a paradigm shift: ASD is not a linear spectrum of severity, but a constellation of discrete neurobiological trajectories
| [4] | Wigdor EM, Gandal MJ, Parikshak NN, et al. Genetic correlates of phenotypic heterogeneity in autism. Nat Genet. 2022; 54: 212-224. https://doi.org/10.1038/s41588-022-01072-5 |
| [10] | Litman A, Sauerwald N, Green Snyder L, Foss-Feig J, Park CY, Hao Y, Dinstein I, Theesfeld CL, Troyanskaya OG. Decomposition of phenotypic heterogeneity in autism reveals underlying genetic programs. Nat Genet. 2025. https://doi.org/10.1038/s41588-025-02224-z |
[4, 10]
. Subtypes with postnatally expressed variants (e.g., Social & Behavioral) may allow later intervention windows, whereas Broadly Affected subtypes show early high-impact de novo variants with severe outcomes
| [7] | Satterstrom FK, Kosmicki JA, Wang J, Breen MS, De Rubeis S, An JY, et al. Large-scale exome sequencing study implicates both developmental and functional changes in the neurobiology of autism. Cell. 2020; 180(3): 568-584.e23. https://doi.org/10.1016/j.cell.2019.12.036 |
| [8] | De Rubeis S, He X, Goldberg AP, Poultney CS, Samocha K, Cicek AE, et al. Synaptic, transcriptional and chromatin genes disrupted in autism. Nature. 2014; 515(7526): 209-215. https://doi.org/10.1038/nature13772 |
[7, 8]
.
Early intervention studies consistently demonstrate benefits
| [13] | Fuller EA, Kaiser AP. The effects of early intervention on social communication outcomes for children with autism spectrum disorder: a meta-analysis. J Autism Dev Disord. 2020; 50(5): 1683-1698. https://doi.org/10.1007/s10803-019-03927-z |
| [14] | Franz L, Goodwin C, Rieder A, Metheis M, Damiano DL. Early intervention for very young children with or at high likelihood for autism spectrum disorder: an overview of reviews. Dev Med Child Neurol. 2022; 64(9): 1063-1073. https://doi.org/10.1111/dmcn.15258 |
| [15] | French L, Kennedy EM. Early intervention for infants and young children with, or at-risk of, autism spectrum disorder: A systematic review. J Child Psychol Psychiatry. 2018; 59(4): 444-458. https://doi.org/10.1111/jcpp.12828 |
| [20] | Gómez-Cotilla R, López-de-Uralde-Selva MA, Valero-Aguayo L. Efficacy of early intervention programmes: systematic review and meta-analysis. Psicol Educ. 2024; 30(1): 1-10. https://doi.org/10.5093/psed2024a1 |
[13-15, 20]
, yet challenges remain in defining which behaviors to target
| [18] | Lin A, Rorvik A, et al. Conceptualizing and measuring ‘problem behavior’ in early childhood in ASD: a systematic review. JCPP Res Pract. 2025; ahead of print. https://doi.org/10.1111/jcpp.14177 |
[18]
and in standardizing culturally sensitive tools. Machine-learning approaches integrating phenotypic and genomic data improve screening accuracy and subtyping
| [19] | Bedford R, Waldmann S, et al. Machine learning of clinical phenotypes facilitates autism screening: insights from AGRE and transcriptomics. Sci Rep. 2025; 15(1): 95291. https://doi.org/10.1038/s41598-025-95291-5 |
[19]
.
Together, current evidence indicates that ASD is best conceptualized as a spectrum of differentiated biological trajectories. Subtyping offers promise for overcoming diagnostic heterogeneity, improving prognosis, and tailoring interventions, though further research must enhance representativeness and translational applicability.
Expanded Limitations
Despite promising progress, several limitations persist. The representativeness of available cohorts remains restricted, with underrepresentation of ethnic and low-income populations. Cross-site heterogeneity in diagnostic tools, behavioral rating scales, and cognitive assessments limits comparability. Additionally, variability in genetic annotation depth and quality constrains reproducibility of genotype-phenotype correlations. Addressing these gaps will require harmonization of study protocols through common data elements (CDEs), shared ontologies, and standardized phenotyping instruments. Equitable inclusion of diverse populations is critical to ensure the global applicability of emerging subtype frameworks.
Future Directions
Future studies should prioritize longitudinal validation of ASD subtypes to assess developmental stability and predictive clinical utility. Pragmatic clinical trials embedding subtype-aware decision tools into healthcare systems are needed to determine feasibility and impact on outcomes. Integration with electronic health records (EHRs) and explainable artificial intelligence (AI) systems will support translation into clinical workflows.
Attention to ethical, cultural, and governance considerations is essential, particularly regarding data privacy, consent, and public engagement. Cross-cultural adaptation of diagnostic and phenotypic instruments must accompany the use of global datasets to prevent disparities in precision medicine applications. Ultimately, collaborative efforts linking genomics, neuroimaging, and behavioral data within transparent, ethically guided frameworks will accelerate the implementation of person-centered care in ASD.
5. Conclusions
The growing recognition of ASD as a heterogeneous condition has driven integrative classifications that combine clinical, phenotypic, and genetic data. Evidence supports the existence of consistent clinical-biological subtypes with distinct behavioral, cognitive, comorbidity, and genomic profiles.
Identifying subtypes through person-centered computational models represents a significant advance toward personalized medicine in neurodevelopment. The finding that certain genetic variants are preferentially associated with specific subgroups, and that their timing of expression differs, suggests that ASD is not a linear continuum but a constellation of distinct biological pathways.
These advances have practical implications, including the development of predictive tools for diagnosis, prognosis, and early intervention. Nevertheless, implementation requires further validation, broader population representativeness, and culturally sensitive strategies that involve the autistic community in the design and evaluation of new tools.
Ultimately, integrating phenotypic and genomic data in large cohorts enables more precise classification of ASD, paving the way for precision medicine in autism. This approach holds the potential to improve prognostic accuracy, personalize interventions, and advance toward equitable, patient-centered care.
Abbreviations
ASD | Autism Spectrum Disorder |
ABA | Applied Behavior Analysis |
SPARK | Simons Foundation Powering Autism Research for Knowledge |
SSC | Simons Simplex Collection |
ADHD | Attention-Deficit/Hyperactivity Disorder |
DSM-5 | Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition |
IQ | Intelligence Quotient |
DNA | Deoxyribonucleic Acid |
SNP | Single Nucleotide Polymorphism |
NGS | Next-Generation Sequencing |
ADI-R | Autism Diagnostic Interview-Revised |
CDE | Common Data Elements |
AI | Artificial Intelligence |
EHR | Electronic Health Record |
Author Contributions
Vicente M. Martinez Cardenas is the sole author. The author read and approved the final manuscript.
Conflicts of Interest
The author declares no conflicts of interest.
References
| [1] |
Lord C, Elsabbagh M, Baird G, Veenstra-VanderWeele J. Autism spectrum disorder. Lancet. 2018; 392(10146): 508-520.
|
| [2] |
Al-Sarraj Y, Taha RZ, Al-Dous E, Ahram D, Abbasi S, Abuazab E, et al. The genetic landscape of autism spectrum disorder in the Middle Eastern population. Front Genet. 2024; 15: 1363849.
https://doi.org/10.3389/fgene.2024.1363849
|
| [3] |
Matoba N, Liang D, Sun H, Aygün N, McAfee J, Davis JE, et al. Common genetic risk variants identified in the SPARK cohort support DDHD2 as a candidate risk gene for autism. Transl Psychiatry. 2020; 10: 265.
https://doi.org/10.1038/s41398-020-00953-9
|
| [4] |
Wigdor EM, Gandal MJ, Parikshak NN, et al. Genetic correlates of phenotypic heterogeneity in autism. Nat Genet. 2022; 54: 212-224.
https://doi.org/10.1038/s41588-022-01072-5
|
| [5] |
Simons Foundation Autism Research Initiative. About SPARK: Simons Foundation Powering Autism Research for Knowledge 2025 Apr 8 (cited 2025 Jul 19). Available from:
https://sparkforautism.org/portal/page/about-spark/
|
| [6] |
Grove J, Ripke S, Als TD, Mattheisen M, Walters RK, Won H, et al. Identification of common genetic risk variants for autism spectrum disorder. Nat Genet. 2019; 51(3): 431-444.
https://doi.org/10.1038/s41588-019-0344-8
|
| [7] |
Satterstrom FK, Kosmicki JA, Wang J, Breen MS, De Rubeis S, An JY, et al. Large-scale exome sequencing study implicates both developmental and functional changes in the neurobiology of autism. Cell. 2020; 180(3): 568-584.e23.
https://doi.org/10.1016/j.cell.2019.12.036
|
| [8] |
De Rubeis S, He X, Goldberg AP, Poultney CS, Samocha K, Cicek AE, et al. Synaptic, transcriptional and chromatin genes disrupted in autism. Nature. 2014; 515(7526): 209-215.
https://doi.org/10.1038/nature13772
|
| [9] |
Al-Beltagi M. Pre-autism: Advancing early identification and intervention in autism. World J Clin Cases. 2024; 12(34): 6748-6753.
https://doi.org/10.12998/wjcc.v12.i34.6748
|
| [10] |
Litman A, Sauerwald N, Green Snyder L, Foss-Feig J, Park CY, Hao Y, Dinstein I, Theesfeld CL, Troyanskaya OG. Decomposition of phenotypic heterogeneity in autism reveals underlying genetic programs. Nat Genet. 2025.
https://doi.org/10.1038/s41588-025-02224-z
|
| [11] |
Wendling P. Four biologically, clinically distinct autism subtypes identified. Medscape Medical News. 2025 Jul 16 (cited 2025 Jul 19). Available from:
https://www.medscape.com/viewarticle/four-biologically-clinically-distinct-autism-subtypes-2025a1000isk
|
| [12] |
Cortese S, Bellato A, Gabellone A, Marzulli L, Matera E, Parlatini V, et al. (2024). Latest clinical frontiers related to autism diagnostic strategies. Cell Reports Medicine, 6(2), 101916.
https://doi.org/10.1016/j.xcrm.2024.101916
|
| [13] |
Fuller EA, Kaiser AP. The effects of early intervention on social communication outcomes for children with autism spectrum disorder: a meta-analysis. J Autism Dev Disord. 2020; 50(5): 1683-1698.
https://doi.org/10.1007/s10803-019-03927-z
|
| [14] |
Franz L, Goodwin C, Rieder A, Metheis M, Damiano DL. Early intervention for very young children with or at high likelihood for autism spectrum disorder: an overview of reviews. Dev Med Child Neurol. 2022; 64(9): 1063-1073.
https://doi.org/10.1111/dmcn.15258
|
| [15] |
French L, Kennedy EM. Early intervention for infants and young children with, or at-risk of, autism spectrum disorder: A systematic review. J Child Psychol Psychiatry. 2018; 59(4): 444-458.
https://doi.org/10.1111/jcpp.12828
|
| [16] |
Vivanti G, Stahmer AC, et al. Can the Early Start Denver Model be considered ABA practice? Behav Anal Pract. 2021; 14(1): 260-269.
https://doi.org/10.1007/s40617-021-00556-x
|
| [17] |
Dong L, Xu B, Wang X, Liu J, Zhang L, et al. Interactions of genetic risks for autism and the broad autism phenotype. Front Psychiatry. 2023; 14: 1110080.
https://doi.org/10.3389/fpsyt.2023.1110080
|
| [18] |
Lin A, Rorvik A, et al. Conceptualizing and measuring ‘problem behavior’ in early childhood in ASD: a systematic review. JCPP Res Pract. 2025; ahead of print.
https://doi.org/10.1111/jcpp.14177
|
| [19] |
Bedford R, Waldmann S, et al. Machine learning of clinical phenotypes facilitates autism screening: insights from AGRE and transcriptomics. Sci Rep. 2025; 15(1): 95291.
https://doi.org/10.1038/s41598-025-95291-5
|
| [20] |
Gómez-Cotilla R, López-de-Uralde-Selva MA, Valero-Aguayo L. Efficacy of early intervention programmes: systematic review and meta-analysis. Psicol Educ. 2024; 30(1): 1-10.
https://doi.org/10.5093/psed2024a1
|
Cite This Article
-
-
@article{10.11648/j.frontiers.20250504.11,
author = {Vicente Martinez Cardenas},
title = {Biological and Clinical Subtypes in Autism Spectrum Disorder: A Review of Recent Advances in Phenotypic and Genetic Classification
},
journal = {Frontiers},
volume = {5},
number = {4},
pages = {159-165},
doi = {10.11648/j.frontiers.20250504.11},
url = {https://doi.org/10.11648/j.frontiers.20250504.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.frontiers.20250504.11},
abstract = {Introduction: Autism spectrum disorder (ASD) is a neurodevelopmental condition characterized by substantial phenotypic and genetic heterogeneity. The recent application of person-centered computational models has allowed the identification of novel clinical subtypes with distinct genetic underpinnings. Objective: To review recent literature on the classification of ASD subtypes through integrative approaches combining clinical, phenotypic, and genomic data, with emphasis on diagnostic, prognostic, and therapeutic implications. Methods: A narrative review of articles published between 2018 and 2024 was conducted in PubMed, Scopus, and Web of Science, using search terms such as “autism subtypes,” “phenotypic clustering,” “genetic architecture in ASD,” and “precision medicine in autism.” Eligible studies included original research, systematic reviews, and meta-analyses. Results: Recent studies have identified at least four robust clinical-biological ASD subtypes using finite mixture modeling and person-centered analyses: (1) social and behavioral challenges, (2) mixed ASD with developmental delay, (3) moderate challenges, and (4) broadly affected subtype. Each group presents distinctive patterns in symptoms, comorbidities, developmental trajectories, and genetic architecture. Both de novo mutations and inherited variants play key roles in molecular differentiation among subtypes. Conclusions: The identification of more homogeneous subgroups within the autism spectrum represents a crucial step toward personalized medicine in ASD. Emerging clinical tools derived from these classifications may enhance prognosis prediction and guide tailored interventions.
},
year = {2025}
}
 Copy
|
Copy
|
 Download
Download
-
TY - JOUR
T1 - Biological and Clinical Subtypes in Autism Spectrum Disorder: A Review of Recent Advances in Phenotypic and Genetic Classification
AU - Vicente Martinez Cardenas
Y1 - 2025/10/30
PY - 2025
N1 - https://doi.org/10.11648/j.frontiers.20250504.11
DO - 10.11648/j.frontiers.20250504.11
T2 - Frontiers
JF - Frontiers
JO - Frontiers
SP - 159
EP - 165
PB - Science Publishing Group
SN - 2994-7197
UR - https://doi.org/10.11648/j.frontiers.20250504.11
AB - Introduction: Autism spectrum disorder (ASD) is a neurodevelopmental condition characterized by substantial phenotypic and genetic heterogeneity. The recent application of person-centered computational models has allowed the identification of novel clinical subtypes with distinct genetic underpinnings. Objective: To review recent literature on the classification of ASD subtypes through integrative approaches combining clinical, phenotypic, and genomic data, with emphasis on diagnostic, prognostic, and therapeutic implications. Methods: A narrative review of articles published between 2018 and 2024 was conducted in PubMed, Scopus, and Web of Science, using search terms such as “autism subtypes,” “phenotypic clustering,” “genetic architecture in ASD,” and “precision medicine in autism.” Eligible studies included original research, systematic reviews, and meta-analyses. Results: Recent studies have identified at least four robust clinical-biological ASD subtypes using finite mixture modeling and person-centered analyses: (1) social and behavioral challenges, (2) mixed ASD with developmental delay, (3) moderate challenges, and (4) broadly affected subtype. Each group presents distinctive patterns in symptoms, comorbidities, developmental trajectories, and genetic architecture. Both de novo mutations and inherited variants play key roles in molecular differentiation among subtypes. Conclusions: The identification of more homogeneous subgroups within the autism spectrum represents a crucial step toward personalized medicine in ASD. Emerging clinical tools derived from these classifications may enhance prognosis prediction and guide tailored interventions.
VL - 5
IS - 4
ER -
Copy
|
Download